
Smile Enhancement in the Era of Minimal Tooth Reduction
By Dimple Desai, DDS, AAACD
There is a constant stream of social media content depicting a wide variety of methods of improving one’s smile. These vary from at-home and in-office tooth whitening to actual dental procedures that alter existing tooth shape and positioning. In many cases, viewing even moderate tooth reduction on these social media platforms can produce anxiety in a patient that is actually contemplating such a dental procedure. Such was the case with a 43-year-old patient whose son was undergoing Invasalign treatment in the office. Due to the abundance of information on social media regarding the aggressive removal of tooth structure in order to improve smile esthetics, she was cautious, even fearful, of seeking dental treatment to improve hers. As she frequented her son’s appointments, she became comfortable enough to broach the subject and inquire as to the possibilities of improving her smile.
The patient’s desire was to have her smile improved by having her teeth longer and look more natural, and in fact presented with maxillary anterior wear (FIG 1A, 1B). Her teeth were scanned, and models were fabricated and mounted. This revealed the moderate wear of the maxillary anterior teeth as well as a constricted bite.


Patient presented with moderate maxillary incisal wear and a desire to have her smile improved with minimal tooth reduction.
The patient subsequently agreed to the treatment plan of Invisalign therapy of approximately 3 months to improve the constricted bite; crown lengthening of teeth #8 and #9 to assist in overall esthetics; and either composite or porcelain veneers on teeth #7 to 10. The patient accepted the treatment plan and readily chose the composite veneer option due to the conservative nature of the tooth preparation, however she was very insistent that as much tooth structure as possible be preserved.
An in-office wax-up was prepared on the mounted models to establish ideal incisal length and thickness as well as lingual and facio-incisal contours. A lingual matrix was fabricated using Template Ultra Quick Matrix Material (Clinician’s Choice) on a model of the wax-up in order to accurately transfer this information to the final restorations. (FIG 2)

A lingual matrix impression of the wax-up is taken using Template Ultra Quick Matrix Material (Clinician’s Choice). This lingual matrix will allow for the accurate transfer of the ideal lingual contour and incisal length and thickness to the final restoration.
The composite chosen was Evanesce due to its optimal handling properties, its high polishability and the absence of any air bubbles upon direct placement onto the tooth. Shade selection was made using a Smile Lite (Smile Line) and placing three triangular samples of three possible shades on a central incisor. These were placed vertically on the facial surface and progressed from thicker to thinner from cervical to incisal then light-cured. These were evaluated under the Smile Lite and Evanesce A1 Universal, B1 Enamel and Enamel White were chosen.
Crown lengthening was carried out on the same day as the composite veneer placement using a surgical blade and a KB chisel. Gingival margins were clean with an absence of any bleeding prior to the placement of the composite. In the event of any threat of blood contamination, a dry retraction cord would have been placed. Tooth preparation of teeth #7–10 was extremely conservative, consisting of discing of the incisal edges and corners and air abrasion of the facial and lingual enamel surfaces. The entire restorative process, including preparation, was carried out one tooth at a time beginning with the central
incisors, followed by the lateral incisors. Isolation was achieved using Optragate (Ivoclar) and a combination of mylar, metal matrices (Kerr Dental), as well as Teflon tape throughout the procedure.
Each tooth was subsequently etched, rinsed and All Bond Universal Adhesive (Bisco), was applied, air dried then light-cured. A small amount of Evanesce Enamel White was placed into the incisal portion of the lingual matrix (FIG 3). This was made as thin as possible using a Composite Ninja (Clinician’s Choice) (FIG 4), then transferred and adapted into place along the lingual margin. This was light-cured prior to removing the lingual matrix.

A small amount of Evanesce Enamel White (Clinician’s Choice) is placed into the incisal portion of the lingual matrix.
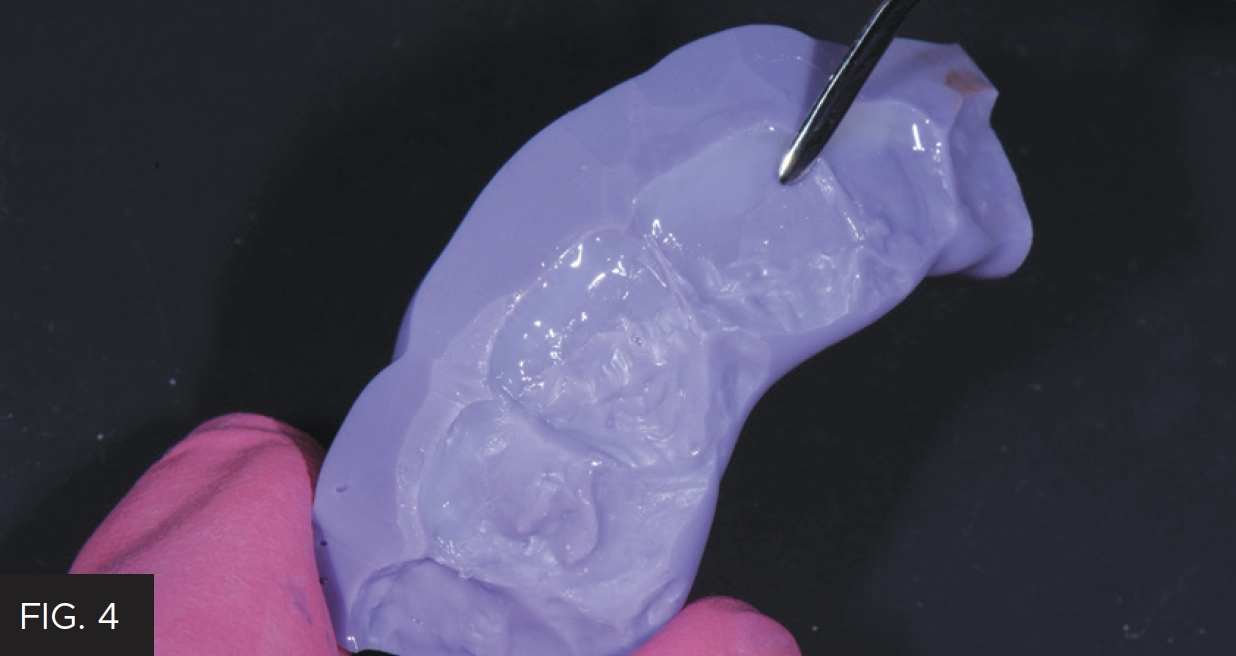
Using a Composite Ninja (Clinician’s Choice), the Enamel White is thinned out as much as possible within the matrix prior to being taken to the prepared teeth and adapted in place.
Subsequent layers of Evanesce A1 Universal and B1 Enamel were then placed, and light-cured in 2-3 increments per tooth. Placement and adaptation to the tooth was achieved using a Composite Ninja (Clinician’s Choice) and OptraSculpt Pads (Ivoclar). Tints were sparingly applied as needed to this layer. A Composculpt #1/2 (Hu-Friedy) instrument was useful in establishing facial lobe development, thus creating depressions for the final layer of Evanesce Enamel Clear to provide the illusion of depth. Each increment and layer of composite was smoothed and blended into the surrounding tooth structure and previous layer using a #3 composite brush (Cosmedent) lightly coated with ResinBlend LV Composite Blending Resin (Clinician’s Choice). (FIG 5)

Prior to light-curing, each layer of composite is smoothed and blended into the previous layer using a #3 Composite brush (Cosmedent) lightly coated with a resin wetting agent, ResinBlend LV (Clinician’s Choice).
The patient’s natural teeth lacked incisal translucency and facial texture and therefore declined having it included in her final restorations. With the lingual contours and incisal length and thickness established in the wax-up successfully transferred from the lingual matrix to the final restorations, only minimal finishing was necessary. The desired facial contours and line angles were traced onto the composite surface with a pencil. Coarse and medium Contours Finishing and Polishing Discs (Clinician’s Choice) were used to shape the composites using the pencil lines as guides. Fine and superfine discs completed the disc sequence. A.S.A.P. Dailies All Surface Access Diamond Polishers (Clinician’s Choice) were used to quickly achieve a very high luster polish. (FIG 6) The purple Pre-polisher was followed by the peach Final High Shine polisher. Each polisher was used with light pressure for 15 – 20 seconds per surface, per tooth.

A.S.A.P. Dailies All Surface Access Diamond Polishers are used to achieve a rapid high luster. The 2-step polishing system starts with the purple Pre-polisher, followed by the peach Final High Shine Polisher (shown above).
Same-day photos were taken, and the patient was thrilled with the esthetic result. Later, upon critical analysis of the clinical photos, it was determined that tooth #8 could be lengthened slightly to better match tooth #9. At the subsequent follow-up appointment, the patient was shown this slight length discrepancy using Keynote. She understood and agreed to this minor change. Once the modification was made to tooth #8, the patient loved the way her smile and bite felt now that it more closely mirrored tooth #9. (FIG 7A, 7B)

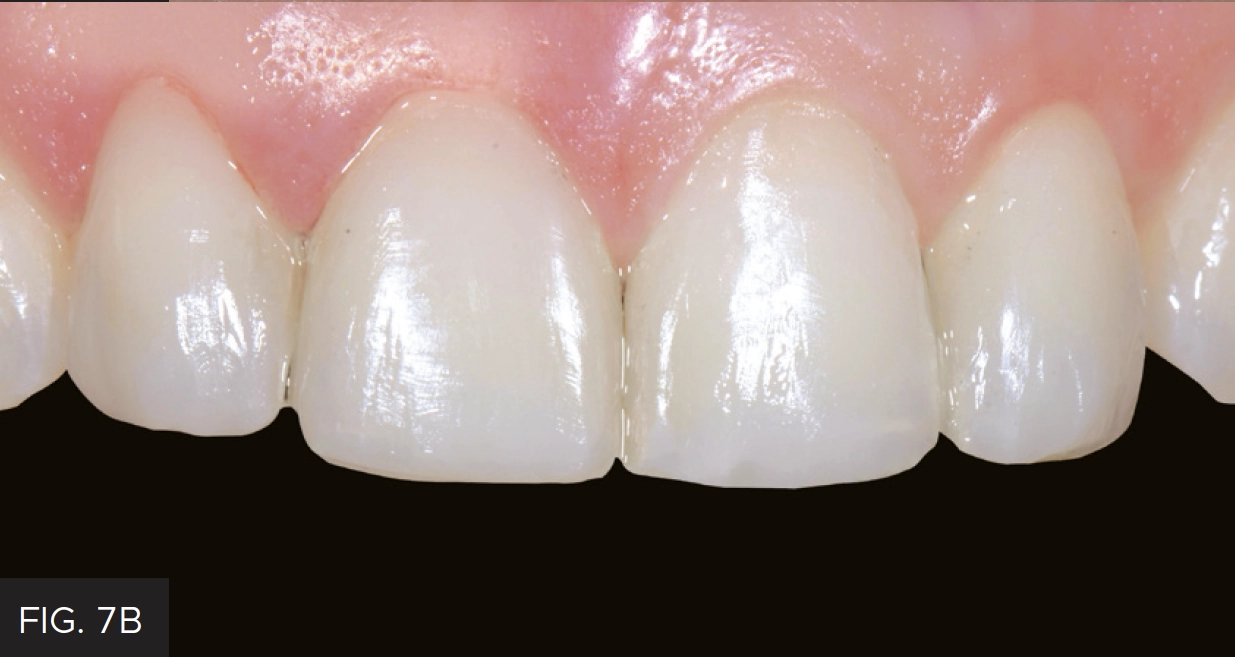
Final composite veneer restorations on teeth #7 through 10 achieved using minimal tooth reduction.
In the end the patient was considerably pleased with her decision to pursue an improvement in her smile, especially given her anxiety at having any tooth structure removed to facilitate it. Throughout the procedure, she required constant assurance that, despite the sound of the handpiece, every attempt at achieving an ultra-conservative solution was being made without compromising the final esthetic result. Social media has had a positive effect on creating interest in improving one’s smile and often steering potential patients into dental offices for clinical evaluations. However, this information can also create a negative opinion, anxiety and fear as to what extent tooth reduction is necessary to satisfy their desire for an improved smile. Composite veneers can provide a long-term esthetic solution without significant tooth structure removal, along with the possibility of an easy repair, repolishing over time to maintain a high luster, and even a possible change shade without complete removal of the restoration itself.

ABOUT THE AUTHOR
Dr. Dimple Desai is the founder of Luminous Smiles of Newport Beach, a boutique dental practice focusing on rejuvenating patients’ lives through their smiles. She has been recognized locally as Orange County’s Top Dentist for the past three years and was selected as one of the Top 40 Dentists under the age of 40 in the country. Dr. Desai obtained both her Bachelor’s degree in Dental Hygiene and a Doctorate of Dental Surgery from the University of Southern California, and later returned to her Alma Mater as a Clinical Adjunct Professor to educate dental students on the clinic floor. Dr. Desai is also a graduate of the Kois Institute and is an Accredited Member of the American Academy of Cosmetic Dentistry.
Share This Article! Choose Your Platform
Products Mentioned in this article




Related Articles

Multilayer Composite Technique for Extraordinary Outcomes in Common Clinical Situations
By Megan Shelton, DMD
Responsible esthetic dentistry embraces the notion of optimizing esthetic results with minimal tooth structure removal while acknowledging the inherent risk to the dentition as a result of any restorative intervention. It is this systemic approach that underlies my esthetic treatment planning and, more often than not, multilayered composite allows me to provide the highest quality esthetic dentistry with the least impact to tooth structure.
A Conservative Approach to Restoring the Worn Anterior Dentition
By Newton Fahl, DDS, MS
Long-term restorative treatment of the worn dentition can be a complex endeavour and possibly extend beyond the scope and experience of the general dentist. Additionally, restoration of this compromised dentition may require other health disciplines’ involvement to address any psycho-social factors that may limit the long-term success of the restorative treatment.

Using Injection Molding Composite Veneers as a Transitional Guide During Orthodontic Treatment
By Megan Shelton, DMD
It is not uncommon for adolescents to exhibit spacing in the anterior dentition and this can often be the motivating factor in seeking orthodontic treatment. Microdontia, the term used to describe teeth that are smaller than normal, is frequently responsible for this spacing and can lead to a Bolton discrepancy when present in one arch relative to the opposing arch.