
Simple Anterior Composite Restorations
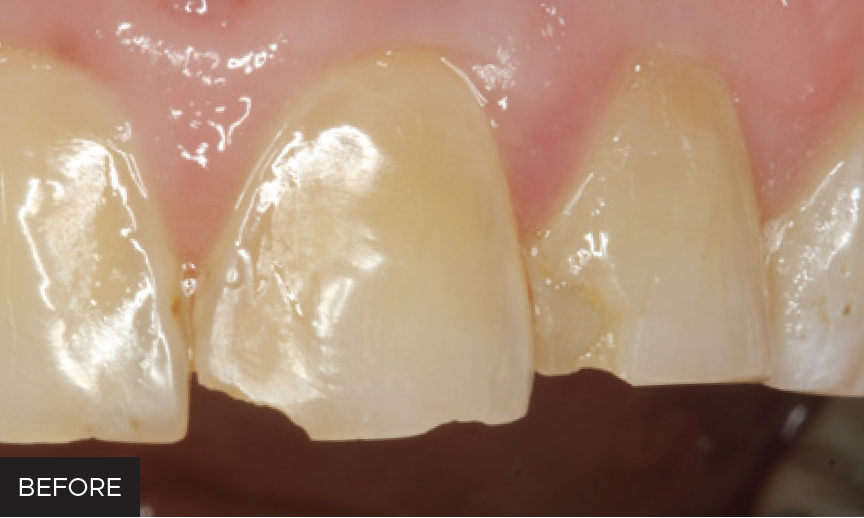
A patient presented to the University of Alabama, School of Dentistry with fractured composites on the mesial incisal edges of his left central and lateral incisors that had been placed 20 years previously. Due to the longevity and his esthetic satisfaction of the previous composite restorations, the patient opted for replacement with direct composite restorations.
Immediately after the patient consented to treatment, a shade of composite was selected. To delay composite shade selection to the point of tooth desiccation can result in selecting a shade that is too high in value (too light). Composite shade was determined by placing a small piece of composite on the tooth of interest and light-curing. This method of shade selection is often more accurate than the use of a shade guide.
Once the shade was selected, a medium gauge nonlatex True Dental Dam (Clinician’s Choice) was placed. The teeth were prepared with a diamond bur, removing all previous composite. A bevel was then placed on facial enamel to assist with enamel bonding and shade blending.
The enamel was etched with phosphoric acid, rinsed, and dried. A universal bonding agent was applied to the tooth and cured. Due to the relative opacity of the tooth and the patient’s low esthetic demands, a single shade of composite was used (B3). A lingual and interproximal shelf was created by wrapping a mylar matrix around the tooth and securing it with a wedge. The rationale for application of a lingual/interproximal layer first is both to respect the depth of cure of the composite and form a structure onto which the facial surface of composite could be applied. This first increment was light-cured.
The facial surface of composite was applied in a single increment. In order to spread the composite, a small brush (Cosmedent #3) was lightly dipped in ResinBlend LV (Clinician’s Choice) composite wetting resin. This wetting agent is an unfilled resin that helps to spread and blend composite. It does not contain a hydrophilic monomer (HEMA), so it should not cause the composite to undergo additional staining, which may occur if bonding agent was used instead. Once the brush was dipped in ResinBlend LV, the composite was easily manipulated. ResinBlend LV created an excellent blend of the composite with the surrounding tooth structure. The composite was then light-cured.
The rubber dam was removed and occlusion was checked. Small adjustments to the lingual of restorations were performed with a football-shaped carbide finishing bur.
For contouring the facial surface, or removing excess composite, a fine finishing diamond or Contours Finishing and Polishing Discs (Clinician’s Choice) can be used. The composites were then finished and polished using A.S.A.P. Dailies (Clinician’s Choice). The Prepolisher (purple) was used first to remove surface roughness. The Final High Shine Polisher (peach) was then used to achieve the final high gloss.


ABOUT THE AUTHOR
Nate Lawson DMD, MA, PhD is the Director of the Division of Biomaterials at the University of Alabama at Birmingham School of Dentistry and the program director of the Biomaterials residency program. He graduated from UAB School of Dentistry in 2011 and obtained his PhD in Biomedical Engineering in 2012. His research interests are the mechanical, optical, and biologic properties of dental materials and clinical evaluation of new dental materials. He was the 2016 recipient of the Stanford New Investigator Award and the 2017 3M Innovative Research Fellowship both from the American Dental Association. He served on the American Dental Association Council of Scientific Affairs and is on the editorial board of The Journal of Adhesive Dentistry and Compendium. He has lectured nationally and internationally on the subject of dental materials. He also works as a general dentist in the UAB Faculty Practice.
Share This Article! Choose Your Platform
Products Mentioned in this article



Related Articles
Creating Natural Restorations for Pediatric Trauma Teeth
By Tiffani Dunn, DMD, AAACD
Developing a systematic approach and mastering the techniques for anterior composite restorations can be a gamechanger for the real-world clinician. There are many different and correct approaches to have a predictable outcome.

Ask the Expert: An Interview with Nate Lawson, DMD, PhD on Universal Adhesives
By Nate Lawson, DMD, PhD
What is an universal adhesive? A “universal” adhesive is not a technical term but rather a clinical term. It implies that an adhesive can be used with or without phosphoric acid on dentin or enamel. In scientific writing, these adhesives are sometimes referred to as mild self-etch adhesives because they have a slightly less acidic pH (around 3) than typical self-etch materials (around 2).

A Stress-free Approach to Tooth Isolation
By Anthony Mennito, DMD
In my opinion, we are in a golden age of dentistry. The materials we have at our disposal are incredibly esthetic, increasingly durable, and can be placed with minimal to no removal of healthy tooth structure. So why are we so stressed out all the time?

Take 5: 5 Restorative Clinicians’ Take on True Dental Dam
5 Restorative Clinicians' Take On True Dental Dam.

Closer Look: True™ Dental Dams Stand Out From the Crowd
By Nate Lawson, DDS, MA, PhD
The Clinician’s Choice rubber dams stand out among others due to their versatility, tear resistance, flexibility, and color.

An Ultra-conservative Path Leads to Unparalleled Patient Satisfaction
By Ellen Katz, DDS
There is a feeling of immense satisfaction when you complete an esthetic case, and the patient cannot stop smiling because you have delivered exactly what they had envisioned. It can be challenging for a patient to communicate what it is that they do not like about their smile, leaving the possibility that the clinician does not completely understand what procedure to perform. It takes active listening, restating, rephrasing, and follow-up questioning to clarify what vague description of dislike for their smile may be.