
An Effective Ceramic Polishing Technique in Everyday Practice
By Fred H. Peck, DDS, FAACD
Placing permanent ceramic restorations in our patients’ mouths is an everyday occurrence for the restorative dentist. These restorations help to restore lost tooth structure, stabilize the occlusion, replace missing teeth, and improve esthetics. The final surface texture must be smooth and polished for patient comfort and to prevent damage to opposing teeth.
The critical parts of finalizing the restoration are ensuring an excellent fit, proper occlusal contacts, desensitization of the prep, proper cementation, and clean-up. The provisional restoration is removed from the tooth and the provisional cement is removed from the tooth surface. The tooth preparation must be adequately cleaned. This is best accomplished with sandblasting the tooth structure with 27-micron aluminum oxide in a microetcher to ensure clean healthy enamel and dentinal surfaces, which will improve bond strength. Prior to cementation the tooth must be desensitized, and the dentinal tubules sealed with a product such as G5 (Clinician’s Choice). G5 is bactericidal and will prevent post-operative sensitivity. All residual cement must be removed and one must prevent tooth desiccation prior to final cementation.
Attention is then directed to the occlusal surface. If occlusion is too low, this would be evident during the try-in phase. At this point, additional ceramic material should be added to the occlusal surface to ensure proper centric stops and no drifting of opposing teeth. This may involve returning the restoration to the lab. However, when occlusion is too high, adjustments must be finalized to obtain a highly polished surface. A rough surface can collect stain, become an irritation to the tongue, and more importantly, cause abnormal wear on the opposing teeth. It has been shown that even a glazed surface from the lab can cause unwanted opposing tooth wear. A hand polished surface is best. The following is a polishing system that is very effective in achieving a highly polished surface on the porcelain restoration chairside.
The A.S.AP. Indirect+ system (Clinician’s Choice) is an excellent choice for polishing zirconia, lithium disilicate and many other ceramic surfaces. (FIG 1)
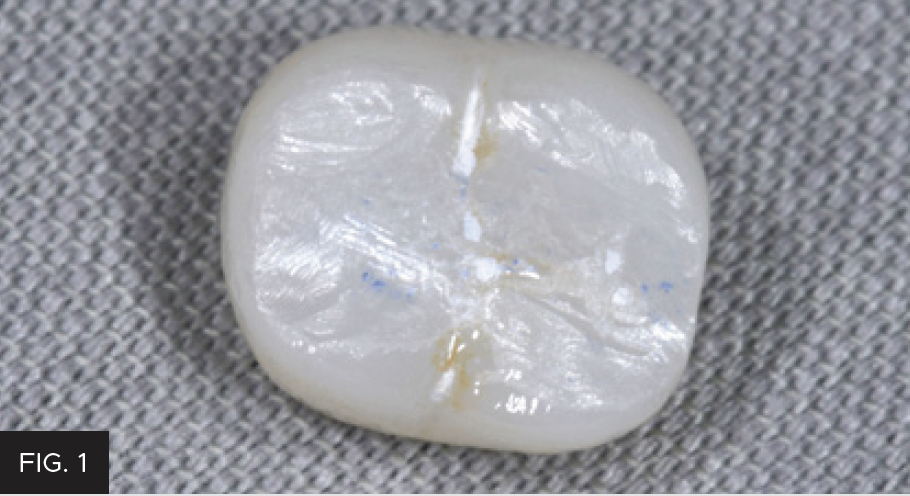
Zirconia crown after diamond bur adjustment.
The A.S.AP. system really is an “all surface access polisher” because the feather edge of the discs allows polishing the smooth surfaces and into deep grooves and crevices. Occlusal verification starts with an 8-micron articulating paper marked in centric and lateral excursions. After the adjustment is completed, often with high-speed burs and finished with an extra fine high-speed diamond, the next step is to use the diamond-impregnated adjusters. (FIG 2)

Diamond-impregnated adjusters intraorally.
They come in three different shapes for adjustment of all the crown surfaces. These adjusters are used to remove the scratches left from the adjustment burs. A moderate amount of hand pressure will remove deeper scratches whereas light pressure will remove the superficial scratches. This takes about 1-2 minutes. (FIG 3)

After use of diamond impregnated adjusters.
Once the scratches are removed and the occlusal contacts are correct, the restoration is then polished. The system includes diamond-impregnated wheel pre-polishers (blue) and final polishers (pink). The polishers come in both intraoral contra angle latch polishers and extraoral lab wheels for a straight nose cone.
Initial adjustments can be done extraorally and after cementation and final verification, the contra-angle polishers and be used intraorally as needed. As with the adjusters, the pre-polishers and final polishers also require light to moderate pressure to finish and polish. The pre-polishers take about 1 minute to smooth the porcelain, and the final polishers take about 30 seconds for a high shine. (FIG 4, 5, 6 and 7)

Use of blue pre-polisher.

After use of blue pre-polisher, dull smooth
surface.

Use of pink final polisher.

After complete polishing, for a high gloss surface.
The adjusters, pre-polishers and final polishers can then be autoclaved to be reused. They have excellent longevity and a low wear rate, allowing them to be used on many patients and many restorations.
Other uses of the A.S.A.P. Indirect+ Polishers are everyday composite restorations, provisional crowns, and removable and fixed hybrid prostheses.
The author suggests after cementation on the most posterior teeth, to check the occlusion using a bi-manual manipulation technique of the mandible. This will ensure the condyle is fully seated in the joint and there are no premature contacts or interferences. The patient will have an excellent ceramic restoration that should last several years.

ABOUT THE AUTHOR
Dr. Fred H. Peck is a third-generation dentist practicing in Cincinnati, OH for over 30 years. He is a graduate of The Ohio State University College of Dentistry and completed his residency at the University of Pittsburgh Medical Center. He is an Accredited Fellow of the AACD, a Fellow of the International College of Dentists, a Kois Center graduate, Dawson Academy graduate and a mentor for Cerecdoctors.com. He has published numerous articles and presented topics at many dental meetings on cosmetic dentistry, dental lab communication and direct resin bonding including hands-on seminars. He is active in the Cincinnati Dental Society and teaches the dental residents at the University of Cincinnati Medical Center. Dr. Fred Peck is in private practice in Cincinnati, OH.
Share This Article! Choose Your Platform
Products Mentioned in this article

Related Articles
Treating Decay Subgingivally with the Bluewave™ Soft Tissue Diode Laser
By Fred Peck, DDS, FAACD
Every day, dentists encounter decay in areas of the mouth where the teeth are a challenge to effectively treat, due to the decay extending beneath the gingival tissue. Saving these teeth is beneficial to the patient in maintaining function and esthetics, even more so if it can be done in a cost-effective manner.

Ask the Expert: An Interview with Dean Vafiadis, DDS on Adjusting and Polishing Zirconia Restorations
How are you currently polishing your zirconia restorations post-adjustment?
Success and Predictable Results with Anterior Composites Every Single Time
By David Chan, DMD, AAACD
The ability to rehabilitate or enhance a smile using direct composite restorations in the esthetic zone can be considered the ultimate challenge for the cosmetic dentist.
Restoring a Lateral Incisor to Proper Dimensions After Orthodontic Treatment
By Danièle Larose, DMD, AAACD
The most conservative method of restoring a Class IV fracture or correcting an anterior tooth size discrepancy is often composite resin.

Facially Driven, Single Opacity Composite Veneers
By Mark Bowes, BDS Rand
Tooth wear has become a common problem, and today it affects both young and old patients. Ceramic veneers have been the standard treatment for many years. However, patients today are looking for more conservative and more cost-effective ways to treat missing, diseased, and unsightly tooth structure.
Simple Concepts to Shape and Polish Anterior Composites to Rival Porcelain
By David Chan, DMD, AAACD
With contemporary direct composite systems, the clinician can now truly be a dental artist by conservatively and esthetically creating restorations that are so life-like that they virtually emulate the beauty of natural tooth structure.