
Increasing Restorative Success Means Making Smarter Choices During Provisionalization
By Douglas Harvey, BSc., DDS and Bob Margeas, DDS
The scope of temporization goes beyond the protection of the prepared tooth. Maintenance of tooth position as well as gingival health and position surrounding the preparation during the provisional phase are just as important for optimal results. These conditions provide the ideal environment for the esthetic evaluation and eventual cementation of the final restoration.
Although there are other factors influencing the quality and durability of the temporary, the choice of your temporary cement should be considered just as carefully as the choice of temporary matrix or temporary material.
One of the key elements in providing for a successful provisional stage is the choice of temporary cement. This choice plays a significant role in determining the condition of the tooth and gingival health at the time of final cementation. An ideal temporary cement should be strong enough to resist the forces of mastication to ensure that the provisional crown or bridge remains in place from the time of preparation until the appointment for the final restoration. However, this retention should be balanced with the ability of the temporary as well as the temporary cement, to be removed with little effort when necessary. Having the temporary in stable position during the provisional phase ensures that the position of the prepared teeth remains identical in the final impression, minimizing any insertion adjustments.
An ideal temporary cement should be non-irritating to the prepared tooth as well as the adjacent marginal gingiva. The temporary cement should also soothe the freshly prepared tooth while providing bacteriostatic properties to prevent gingival inflammation, maintaining a healthy and esthetic environment for final cementation. Furthermore, the temporary cement should not interfere with your ability to cement or bond the final restoration in any manner you may choose.
Besides meeting these requirements as it relates to the material’s physical properties, the ideal temporary cement should be easy and predictable to mix chairside with an adequate working time and a relatively short set time. Additionally, any excess cement around the provisional restoration must be easily and completely removed. This is essential to not only save valuable chair time, but to prevent small residual particles of temporary cement left near or in the gingival sulcus. The presence of such particles poses a risk of forming inter-appointment gingival inflammation, something that can be detrimental to the successful delivery of the final restoration.
THE WORKFLOW
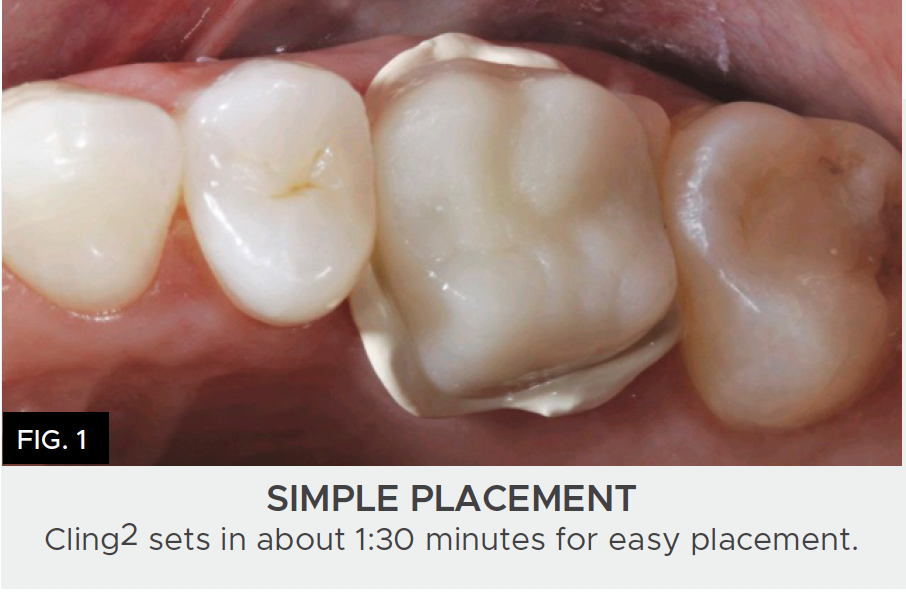
Cling2® Resin Optimized Temporary Cement from Clinician’s Choice® was designed to provide predictability and convenience for all your provisional cases. Cling2 comes in an automix 5mL or 10mL syringe and 25mL cartridge kit configurations that make for easy mixing and placement inside the temporary restoration. (FIG. 1)
With an adequate 30-second working time and an efficient 90-second set time, chair time is minimized and excess cement is easily removed, often flaking off in chunks from the margins, reducing the possibility of trapping small particles subgingivally. (FIG. 2)

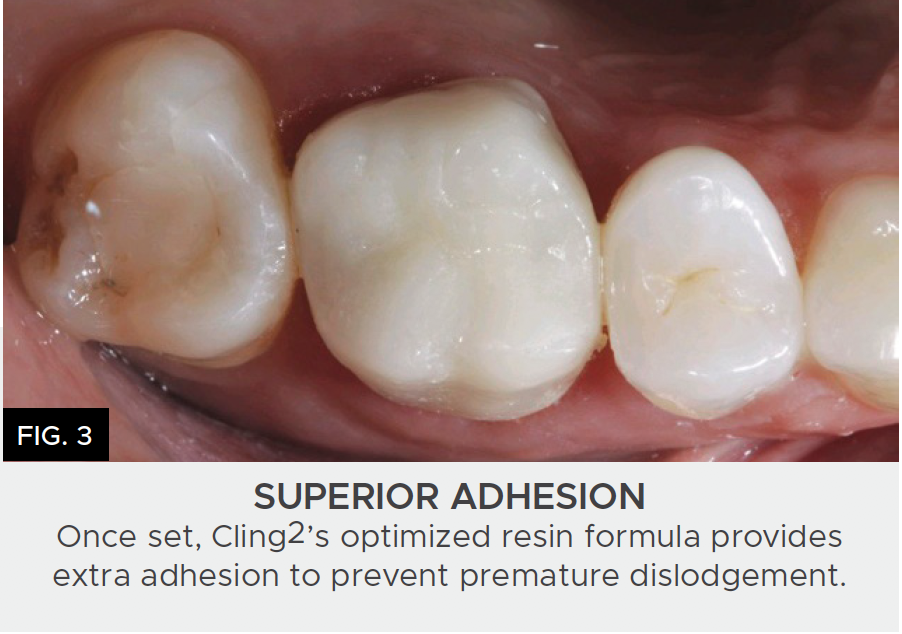
The Cling2 non-eugenol formula soothes and protects the prepared tooth while ensuring the prepared surface is contaminant-free. The addition of a small amount of polycarboxylate resin in the Cling2 formula results in a more retentive temporary restoration, which prevents the provisional from detaching between appointments, yet is easily removed when necessary. (FIG. 3) The presence of polycarboxylate resin also enhances the marginal seal and produces less cement washout for a more comfortable temporary restoration.
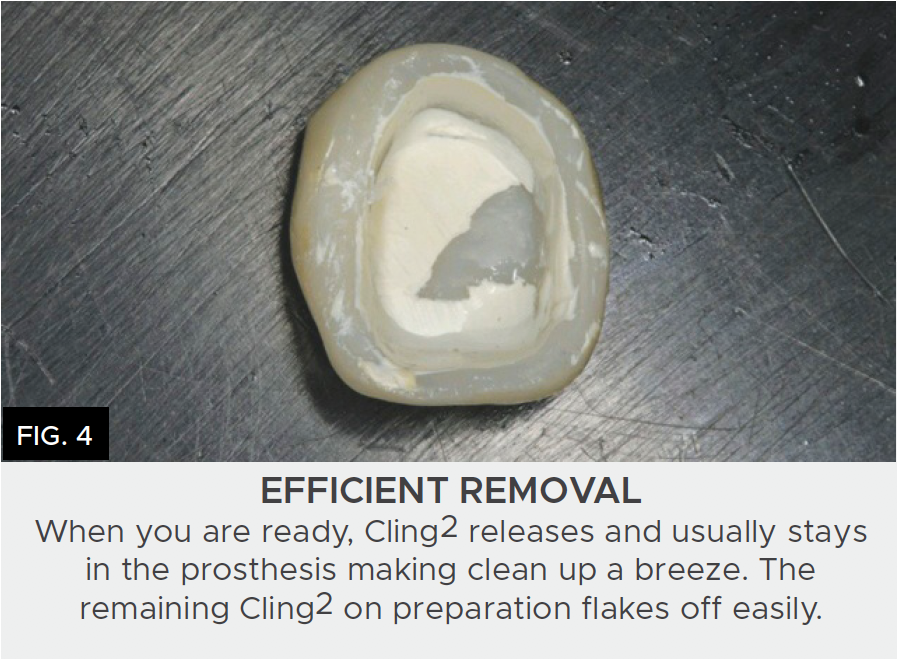
Consider taking less than a minute to polish the temporary with the two-step, one-shape A.S.A.P.® Polishers (Clinician’s Choice®) or applying light-cured Glisten™ Provisional Resin Glaze (Clinician’s Choice®). This will greatly aid in excess Cling2 breaking off in large pieces as well as increasing patient comfort and tissue health. Upon removal, most of the cement will remain within the temporary, leaving very little to clean off of the preparation. (FIG. 4)
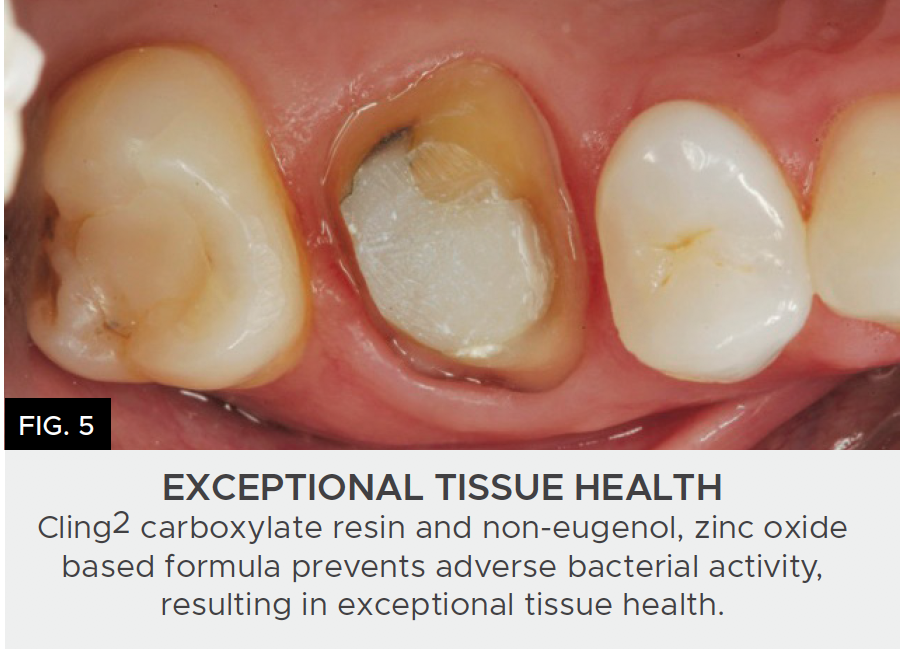
The antibacterial properties of Cling2 reduces gingival plaque retention and is a non-irritant to the tissue itself. It is this ability of Cling2 to heal and maintain the health and position of gingival tissue around the margins of the preparation that allows for a comfortable, esthetically pleasing final restoration. (FIG. 5)
CONCLUSION
Providing your patient with a comfortable, functional, and esthetic provisional restoration does not have to be a complex or time-consuming task. Although there are other factors influencing the quality and durability of the temporary, the choice of your temporary cement should be considered just as carefully as the choice of temporary matrix and temporary material. Cling2 Resin Optimized Temporary Cement provides the necessary retention for a provisional period free of temporary pop-offs while protecting the hard and soft tissues, increasing your predictability of restorative success.

ABOUT THE AUTHOR
Dr. Douglas Harvey is a consultant in Clinical Affairs with Clinician’s Choice Dental Products. He has a Bachelor’s Degree in Biology and a Doctor of Dental Surgery, both from the University of Western Ontario. He served as a dental officer at the Canadian National Defence headquarters before enjoying a career in solo general practice until 2015. Dr. Harvey has been a long-standing member of the International Dental Study Club, and has served in organized dentistry at the local and provincial levels in Canada.

ABOUT THE AUTHOR
Dr. Bob Margeas graduated from the University of Iowa College of Dentistry in 1986 and completed his AEGD residency the following year. He is currently an adjunct professor in the department of Operative Dentistry at the University of Iowa. He is Board Certified by the American Board of Operative Dentistry. He is a Diplomate of the American Board of Aesthetic Dentistry, a Fellow of the Academy of General Dentistry, American Society for Dental Aesthetics and International Team of Oral Implantologists (ITI). He has written numerous articles on esthetic and implant dentistry, and lectures and presents hands-on courses nationally and internationally on those subjects. He is currently the Editor in Chief of Inside Dentistry, on the Editorial Board of Compendium. Dr. Margeas maintains a full-time private practice focusing on comprehensive restorative and implant dentistry.
Share This Article! Choose Your Platform



Related Articles

Predictable and Efficient Single Unit Crown Restorations
By Bob Margeas, DDS
A 55-year-old patient presented to my office with tooth pain upon biting from his second bicuspid. Upon further examination a crack was noted on the mesial marginal ridge.